Thyroid Ultrasound
Fine Needle Aspiration of Thyroid Nodules or Lymph Nodes (FNA)
Thyroid Cyst Aspiration
Thyroid Cyst Ethanol Ablation
Thyroid Nodule Radiofrequency Ablation (RFA)
Laboratory Testing for Thyroid Related Blood Work
Neck Ultrasound for Parathyroid Adenoma Localization
Laboratory Testing for Parathyroid Related Blood Work
Breast and Axillary Ultrasound
Breast Cyst Aspiration
Excision of Simple Breast Lesions
Treatment of Breast Abscess
Removal of Mediport
Placement of SAVI Device for Radiation
BRCA genetic testing
Overview
Fine Needle Aspiration (FNA) is a method by which a mass is determined to be malignant or benign. In a procedure similar to a blood draw, a small needle is placed under ultrasound guidance into the mass and fluid, blood, and cells are removed. The cells are placed on microscope slides to be stained by a pathologist and examined under a microscope. Any remaining fluid is placed in special cytology fluid so that the pathologist has the ability to centrifuge, or spin down the cells, for additional examination. After looking at all the slides, the pathologist will make a diagnosis and issue a written report. The determination of what to do next will determine on the results of that report and individual consultation with the doctor.
How to Prepare for FNA
The procedure itself is quite simple with most of the preparation being in the mind of the patient. If the patient knows that a biopsy is planned, taking a Tylenol ahead of time might be a good idea. If the patient routinely takes prescription medication for anxiety for other medical or dental procedures, that is fine as long as another driver is present. It is best to wear an open necked shirt and not wear necklaces. If hair is long, it is best in a ponytail or braid. Make up or sunless tanner is best removed or have the thought that it will be removed by the doctor prior to the procedure. It is not necessary to fast from food or drink or stop any prescribed medications.
The Actual Procedure
An ultrasound of the targeted area will first be performed to confirm the mass in question. The patient will be repositioned so that the mass may be optimally approached. If the mass is in the neck, a pillow will be used to achieve hyperextension of the neck if possible. The doctor will have the ultrasound probe in one hand and a device that contains the needle in the other. The patient will feel firm pressure from the probe, which is also helping to prevent the mass from moving around. There will be a tiny short lived sharp sensation as the needle enters the mass then a pressure sensation. Patients who are having the procedure done at the neck will report a referred sensation of pressure into the ear or jaw. About 2-3 drops of blood is required for adequate diagnosis. The needle will move back and forth until those drops are collected. It is fine to swallow if necessary. It is impossible to tell someone not to swallow because then they cannot help but have to do so. It is best for the patient not to talk during the procedure. Breathing should be kept shallow, no great sighing or deep yoga type breaths. After the specimen is collected, the needle is removed and light pressure is applied. Unless absolutely necessary, usually only one stick is necessary. Band aid will then be given for sympathy. Mild bruising may occur afterwards, particularly if the patient takes blood thinning medication. There is no reason to alter normal daily activities following the procedure.
Understanding the Results
Typically, results from pathology take 48 business hours. The patient will be called with results. In the event of a benign result and if the doctor does not have any clinical concern based on ultrasound appearance, the recommendation will be typically to follow the mass with another examination (not necessarily another biopsy) in 6 months’ time to assess for growth. If there is concern regarding pathology findings or if there is discordance between the pathology impression and doctor’s impression, the patient will be given the opportunity to come back to the office to discuss. It can be normal for the patient to want to have an extended discussion immediately, but it has been the impression over the years that it is best to allow time for the information to settle and then reconvene with a list of questions. Often times, the last word that a patient hears is “cancer” and then they cannot process any further information at that moment.
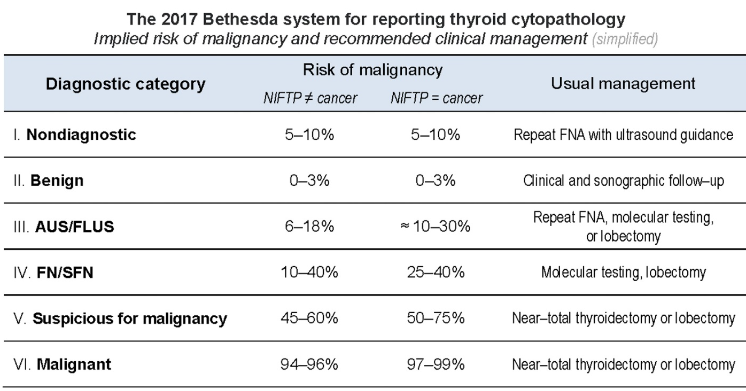
The Bethesda Classification for Thyroid Nodules
For breast masses and lymph nodes, the pathology report is pretty straightforward and patients can move forward based on the results. Thyroid nodules are different. To prevent false positive results (the patient is told that they have cancer and they do not), a pathologist will have a strict check list in which all components must be met before diagnosis of thyroid cancer. In the event that there are some suspicious features but not enough to diagnose cancer, the pathologist will assign a diagnostic category scoring from I-VI. This is called the Bethesda Classification and is a way of standardizing reports. In Bethesda I, the pathologist did not have enough cells to examine either because of blood contamination or presence of clear cyst fluid. In Bethesda II, the biopsy is completely benign and the patient is reassured. Bethesda VI is absolutely cancer. Note, then, that there are 3 categories (III, IV, and V) between benign and malignant, with increasing cause for concern. These categories do not represent an inconclusive biopsy. The pathologist is trying to communicate the presence or absence of atypical cells and assigning a risk of potential malignancy. Bethesda III is named Atypia of Undetermined Significance. Bethesda IV is a Follicular Neoplasm and Bethesda V is more simply called Suspicious for Malignancy. In these situations, it will be an individual discussion between doctor and patient what course of action might be best. There are established recommendations, but each situation is unique to the patient. The situation includes both the clinical findings, presence of concurrent compressive symptoms, and personal feelings of the patient. Options might include ultrasound surveillance over time, repeated FNA, diagnostic thyroid lobectomy (surgical removal of that part of the thyroid with intraoperative biopsy), or removal of the entire thyroid gland. It is important to note that FNA cannot spread cancer cells or “seed” the biopsy tract. Needle aspiration has been used for over 80 years and there is yet to report a single case of such spread.
Ethanol Ablation of Thyroid Cysts
Cysts are either entirely or mostly fluid filled structures within the thyroid. Simple aspiration, or removal of the fluid, may have a high recurrence rate. Ethanol of high purity (95%) may be used to cause tissue damage of the cyst wall to cause collapse of the cyst and reduction in volume. Ethanol works in two ways. It causes a coagulative necrosis of the cyst by causing cell dehydration and protein denaturation. It also causes ischemic necrosis due to interruption of the small blood vessels feeding the cyst. Typically, for an ablation, the cyst fluid is removed and about 50% of volume is replaced by ethanol. The amount can be tailored to the size of the cyst. The procedure is very rapid and is done in the office under ultrasound guidance. Patients may expect at least a 50% decrease in the size of the cyst. This can be a very attractive option for large cysts that cause visible cosmetic defect to the neck. Very large cysts may need more than one ablation. The ablation avoids surgery and has almost no risk of causing hypothyroidism. Patients may experience mild discomfort during the instillation of ethanol and for a day or two after.
Radiofrequency Ablation of Thyroid Nodules
A thyroid nodule is a solid or mostly solid mass within the thyroid. Cancerous nodules are usually removed with surgery. If a patient would have a benign solid nodule, they have several options. They may observe the nodule with ultrasound, remove the nodule with surgery, or ablate the nodule. Radiofrequency Ablation (RFA) is a well-studied and widely used technique using thermal energy to cause tissue necrosis and fibrosis. Although widely used in Europe, it has gained recent acceptance in the US for use in the thyroid. Ablation will not remove the nodule, but it will cause reduction in size. This is particularly important when the nodule is causing compressive symptoms in the neck or is causing cosmetic defect. Sometimes more than one ablation may be necessary for very large nodules.
Before consideration of RFA, it is important that the nodule be proved to be benign. This may require one or two ultrasound guided fine needle aspirations, or biopsies, to make sure. The patient may not be pregnant or have a pacemaker. RFA is typically done under local anesthesia with a mild sedative, unlike the general anesthesia of surgery. Ultrasound is used to guide a probe into the nodule and the tissue is heated until it dies. The probe is moved to as many points within the nodule as possible. This is very similar to the biopsy procedure. A special monitor is used to tell the surgeon when the tissue is dead and when the needle should be moved to living tissue. A cooling pump ensures that heat is only directed at the very tip of the probe to minimize damage to other surrounding structures. The procedure is usually under 30 minutes, but time is taken for education, positioning, local anesthesia, and recovery.
The positive of RFA is that it is not surgery. There is no scar. Recovery is faster. There is almost no risk of hypothyroidism, as there can be with removal of even some of the thyroid tissue.
The risks of RFA are similar to surgery but lessened as it is less invasive. There are still risks of swelling, bruising, temporary difficulty swallowing, and injury to voice nerve causing hoarseness. Patients may experience a sensation of heat in the neck and hear or feel a popping noise (like popcorn) as the tissue heats. Thyroid function is checked several weeks after to ensure that the rest of the thyroid has continued to function normally. The nodule will experience the greatest decrease in size the first month but will continue to shrink a little more over time.
The downside of RFA is insurance coverage. At present, the procedure has not been assigned a CPT code, or code universally recognized by insurance companies for reimbursement purposes. This will likely change in the future as more physicians perform this procedure. However, there are many costs associated with surgery, not just the surgical fee. RFA will save the cost of facility (a surgery center or hospital) and anesthesia, which can usually range into the thousands of dollars. It is usually not necessary to take more than a day off of work, which can also save money.
The decision of what type of treatment is best for thyroid nodule is a mutual decision between patient and physician.